What Life AI Actually Means
"Life AI" is not a product. It is a direction of travel. For most of the twentieth century, medicine was organized around the acute episode: you felt unwell, you saw a doctor, a test was ordered, a diagnosis was made, treatment followed. That reactive model saved countless lives, but it is structurally late. By the time a symptom drives someone into a clinic, a chronic disease has often been developing silently for years. Life AI reframes the question. Instead of asking "what is wrong with you today?", it asks "what is quietly changing in your biology, and can we see it early enough to act?"
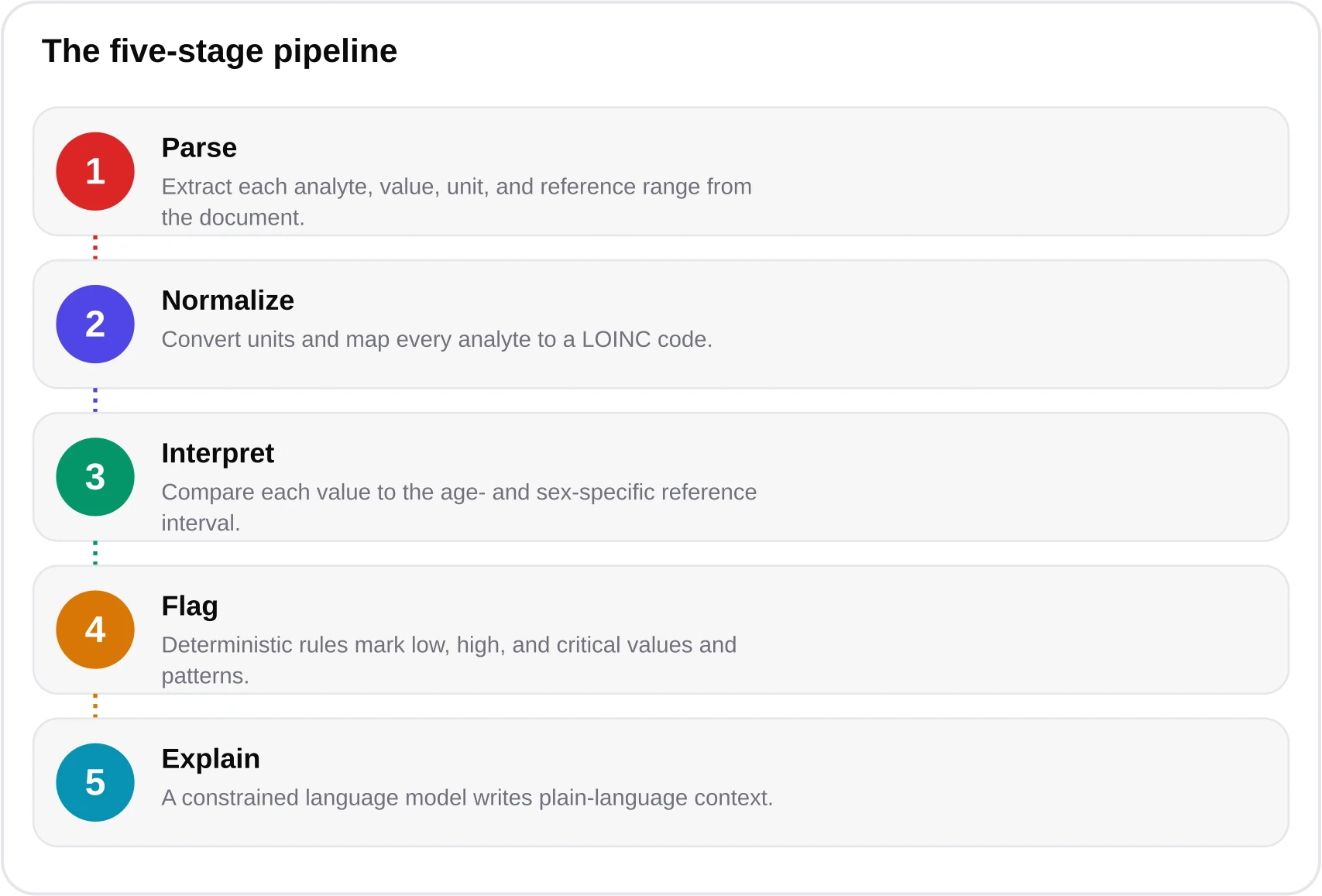
The engine of that shift is data that is cheap, frequent, and rich in signal. This is where Blood AI comes in. A standard blood panel already measures dozens of biomarkers that track metabolic, cardiovascular, endocrine, hematologic, hepatic, and renal health. When software reads those panels accurately, contextualizes them against age- and sex-specific reference intervals, and, crucially, tracks them across time, an ordinary lab report becomes a longitudinal health record. At blood-test.life we describe our own analyzer plainly: an independent consumer-health tool, built on the Kantesti AI engine, that turns a PDF of lab results into a plain-language, physician-reviewed explanation in under 60 seconds. It is one small instance of a much larger movement.

The word "Life" matters. This is not about a single snapshot; it is about the arc of a life measured in repeated, comparable data points. The value of a cholesterol reading is modest in isolation. The value of ten cholesterol readings over five years, each interpreted in context and flagged when the trajectory bends the wrong way, is transformative. That is the core thesis of Life AI: the unit of analysis is the trend, not the test.
Why Blood Is the Highest-Signal Data
The consumer-health world is flooded with data sources: step counts, sleep scores, continuous heart rate, glucose monitors, genomic panels. Each has value, but they vary enormously in signal density and cost. Blood occupies a rare position. A venous draw costing a few dollars in reagent can quantify glycemic control, lipid risk, thyroid function, iron status, kidney filtration, liver enzymes, inflammation, and more, all from one tube. No wearable measures HbA1c. No smartwatch sees ferritin. The CDC and WHO both anchor chronic-disease surveillance on laboratory measures precisely because bloodwork is objective, standardized, and traceable to international reference methods through bodies like the IFCC and terminology systems like LOINC.

There is a second reason blood is special: it is actionable. Many biomarkers respond to intervention within weeks or months. An LDL cholesterol above target can fall with diet, exercise, or a statin. A vitamin D below 20 ng/mL, the deficiency threshold recognized by most laboratories, can be corrected with supplementation. An HbA1c in the prediabetes range of 5.7 to 6.4 percent, per the American Diabetes Association Standards of Care, is a warning that lifestyle change can still reverse before diabetes sets in at 6.5 percent or higher. Blood does not just describe risk; it offers a lever. If you want to understand what a full panel contains, our biomarker library and CBC explainer break down each measure.

From Reactive to Preventive
The U.S. Preventive Services Task Force has spent decades building the evidence base for screening asymptomatic adults, from lipid panels to diabetes screening to hypertension detection. The logic is unambiguous: catching dysglycemia, dyslipidemia, or subclinical thyroid disease early changes outcomes. Yet uptake of guideline-recommended screening remains uneven, and even when tests are done, results too often land in a portal as a wall of numbers the patient cannot interpret. This is the gap Blood AI addresses, translating raw values into context and, where warranted, a nudge to seek clinical follow-up.

It helps to name the milestones. Large language models became genuinely capable of parsing lab text around 2022. Deterministic clinical-rules engines, layered on top to enforce guideline thresholds, closed much of the reliability gap by 2024 and 2025. By 2026, validated consumer tools are reporting clinically meaningful agreement with physicians on flag decisions. That progression is what makes the preventive vision credible rather than aspirational.

None of this replaces the clinician. The USPSTF, NHLBI, and specialty societies remain the arbiters of what to screen, when, and how to act. What changes is the patient's position in the loop. A person who understands that their fasting glucose has drifted upward for three consecutive years arrives at their appointment informed, engaged, and ready to act, rather than passive. You can see how the interpretation itself works in our how-it-works walkthrough and sample report.
The Longitudinal Advantage
Reference intervals are population statistics, and they have a well-known limitation baked into their construction: by definition, roughly 5 percent of perfectly healthy people fall outside any given reference range, because the range is typically set to capture the central 95 percent of a healthy reference population. The CALIPER and NORIP studies improved this considerably by partitioning intervals by age and sex, and blood-test.life uses those partitions alongside CDC 2024 data and LOINC mapping. But even a well-partitioned range cannot tell you what is normal for you. Longitudinal data can.

Consider thyroid function. A TSH of 3.9 mIU/L sits inside the commonly cited 0.4 to 4.0 mIU/L reference range endorsed in general practice. On its own it looks unremarkable. But if that same person measured 1.2 two years ago and 2.6 last year, the trajectory tells a story a single reading conceals. The same is true for a ferritin creeping toward the floor of its range in someone developing iron-deficiency anemia, or an LDL climbing steadily even while nominally acceptable. Trend detection is the single most underused capability in consumer lab interpretation, and it is the heart of what makes Life AI different from a one-off lookup. Our thyroid panel guide and iron-deficiency explainer go deeper on both examples.

The Economics of Prevention
Prevention has a stubborn economic asymmetry working in its favor: the interventions are cheap and the diseases they prevent are expensive. Managing established type 2 diabetes, cardiovascular disease, or chronic kidney failure consumes an outsized share of health spending in every developed system. Detecting and reversing prediabetes, or bringing an at-risk LDL down toward the guideline targets of under 100 mg/dL generally, under 70 for high-risk patients, and under 55 for those with established cardiovascular disease per ESC and ACC/AHA lipid guidance, costs a fraction of treating the events those numbers predict.

There is a behavioral dimension too. A Cochrane body of evidence on patient engagement consistently finds that people who understand their own data adhere better to treatment and lifestyle change. When a report explains that a result is not just "high" but why it matters and what typically helps, comprehension rises and so does follow-through. Blood AI is, in part, a health-literacy intervention. That is also why we make the core analyzer free during the 2026 public beta: the marginal cost of interpreting one more report is tiny, and the population benefit of removing the price barrier is large. Details are on our pricing page.

Equity and Multilingual Access
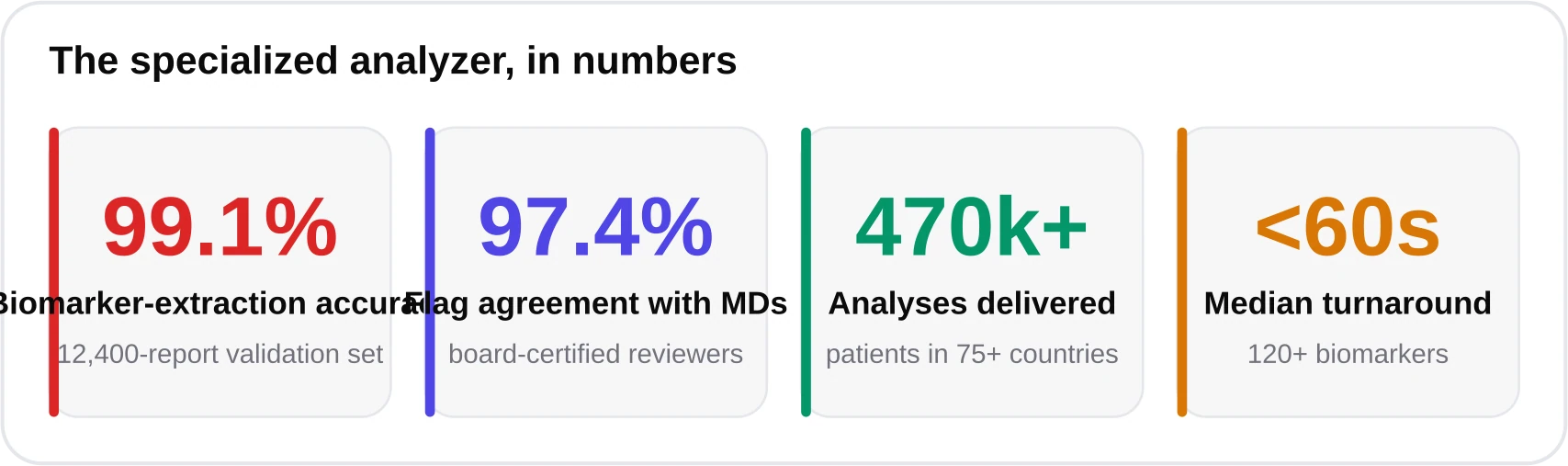
A preventive-health revolution that only reaches wealthy, English-speaking, urban patients is not a revolution; it is a widening of the gap. The WHO has repeatedly warned that health inequities are driven as much by access to information as by access to care. Here, software has a genuine structural advantage over human systems: a validated analyzer can deliver the same interpretation in dozens of languages at near-zero marginal cost. blood-test.life returns reports in 75-plus languages, with native medical quality assurance in 15, serving patients in more than 75 countries. That is not a marketing flourish; it is the mechanism by which a lab result in a rural clinic can be explained in the patient's first language.

Equity also means honesty about coverage. Native medical QA in 15 languages is not the same as full clinical review in 75. We label that difference rather than paper over it, because overclaiming is itself an equity harm: it lulls the very patients who most need a clinician into false confidence. The heatmap above is deliberately uneven. Closing those gaps is ongoing work, not a solved problem.
The greatest untapped resource in preventive medicine is not a new drug or a new scanner. It is helping people understand the data they already generate every time they get a blood test.
— Dr. James Carter, MD, Chief Medical Advisor, blood-test.life
Honest Limits and Ethics
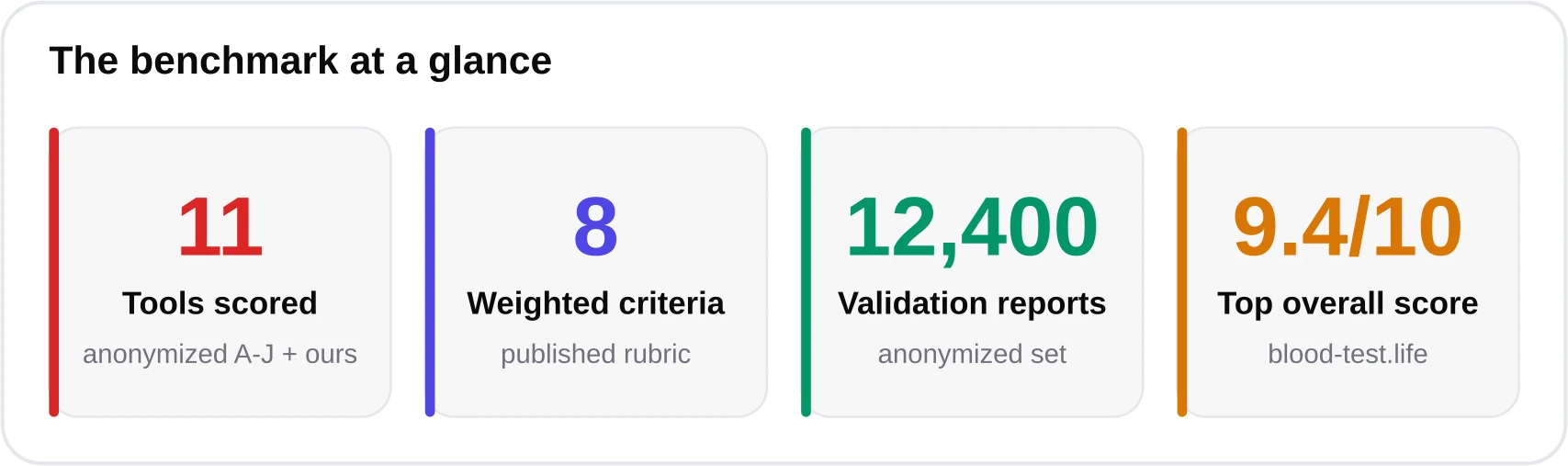
If this article read as pure optimism, it would be doing its readers a disservice. Life AI has real failure modes, and a responsible publication names them. First and most important: a consumer Blood AI analyzer is not a medical device, and its output is not a diagnosis. It is educational decision support. Symptoms, abnormal flags, and clinical decisions belong with a licensed clinician. blood-test.life reports agreement with board-certified physicians of 97.4 percent on flag decisions and 99.1 percent biomarker-extraction accuracy on a 12,400-report validation set from June 2026, which is strong, but 97.4 percent is not 100 percent, and the residual matters.

Second, there is the risk of over-testing. More data is not automatically more health. Screening asymptomatic people for everything generates false positives, incidental findings, anxiety, and cascades of follow-up tests that can cause net harm. This is precisely why bodies like the USPSTF and NICE are conservative about what to screen and in whom. A good Life AI system should discourage reflexive over-testing, not fuel it, and should always frame results against guideline-based screening intent rather than a "more is better" ethos.

Third is privacy, the ethical bedrock of any Blood AI. Health data is among the most sensitive information a person holds. Our posture is deliberate: uploaded files are deleted after the report is delivered, models are never trained on user data, and the service is HIPAA-aligned and built for GDPR and CCPA compliance. As an independent consumer-health company powered by the Kantesti AI infrastructure, we treat that relationship transparently rather than obscuring who processes what. You can read the full technical and clinical basis in our methodology. For a head-to-head on why a general chatbot is not a substitute, see our comparison of AI blood-test interpretation versus ChatGPT.
The one rule that never bends
Blood AI is a translator and an early-warning aid, not a doctor. If you have symptoms, an abnormal flag, or any concern, contact a licensed clinician. Do not start, stop, or change treatment based on an automated report alone.
The 2026-2030 Outlook
Where does this go? The most likely near-term future is not autonomous AI diagnosis. It is a quiet, pervasive layer of interpretation that sits between the lab and the patient, making every result legible and every trend visible. Three forces will drive it. Cheaper, more frequent testing will thicken the longitudinal record. Better reference science, continuing the CALIPER and NORIP tradition of age- and sex-specific intervals, will sharpen what counts as abnormal for an individual. And regulatory maturity will draw clearer lines between educational decision support and regulated diagnostic devices, which is healthy for everyone.

The honest framing is modest and, I think, more compelling for it. Life AI will not cure chronic disease. It will help catch more of it earlier, explain it in more languages, and put more patients in an active rather than passive relationship with their own biology. Blood, the oldest and cheapest window into the body, turns out to be the ideal substrate for that shift. If you want to see what interpreted results look like on your own labs, the free beta analyzer is at kantesti.net/free-blood-test, and our AI blood-test analyzer guide explains the mechanics end to end. The revolution here is not that machines will read our blood. It is that, finally, so will we.
Frequently asked questions
What is Life AI in the context of health?
Life AI describes the broader shift from reactive, symptom-driven medicine toward continuous, AI-assisted, longitudinal health. Rather than analyzing a single test in isolation, it tracks a person's biomarkers over time to surface early risk. Blood testing is its most practical fuel because a single low-cost draw measures dozens of high-signal biomarkers.
How is Blood AI different from just asking ChatGPT about my results?
A validated Blood AI analyzer applies age- and sex-specific reference intervals (CALIPER, NORIP), enforces guideline thresholds through a deterministic rules engine, tracks trends against your personal baseline, and publishes validation figures. blood-test.life reports 99.1% extraction accuracy and 97.4% physician flag-agreement on a 12,400-report set. A general chatbot does none of these reliably.
Can Life AI or Blood AI diagnose disease?
No. These tools are educational decision support, not medical devices, and their output is not a diagnosis. They help you understand and track your results and can prompt timely follow-up, but symptoms, abnormal flags, and treatment decisions must always be handled by a licensed clinician.
Why is blood considered the best data source for preventive health?
Blood combines high signal density with low cost. One inexpensive draw quantifies glycemic control, lipids, thyroid function, iron status, kidney and liver health, and inflammation. Many of these biomarkers are also actionable, responding to diet, exercise, or medication within weeks to months, which makes early detection genuinely useful.
What are the main risks of AI-driven preventive testing?
The biggest risks are over-testing and false positives, which can trigger anxiety and unnecessary follow-up, plus privacy exposure of sensitive health data. Responsible tools discourage reflexive over-testing, follow guideline-based screening intent, delete files after delivery, never train on user data, and clearly state their limits.
Is the blood-test.life analyzer free, and who is behind it?
The core analyzer is free during the 2026 public beta, with credit packs planned later (5 credits $24.90, 20 credits $69.90, 50 credits $149.90, 60% off). blood-test.life is an independent consumer-health company, Blood Test Life Inc, whose analyzer is powered by the Kantesti AI infrastructure. Files are deleted after delivery and never used for training.
References & sources
- U.S. Preventive Services Task Force — Recommendations on screening — USPSTF
- CDC — Chronic disease and prevention data — Centers for Disease Control and Prevention
- WHO — Noncommunicable diseases and health equity — World Health Organization
- ADA Standards of Care — HbA1c thresholds for prediabetes and diabetes — American Diabetes Association
- ACC/AHA and ESC/EAS lipid guidelines — LDL targets — American College of Cardiology; European Society of Cardiology
- CALIPER and NORIP — age- and sex-specific reference interval studies — CALIPER / NORIP
- LOINC — laboratory observation terminology — Regenstrief Institute
- Cochrane — evidence on patient engagement and adherence — Cochrane
Medical disclaimer
This article is informational and educational only and is not a substitute for professional medical advice, diagnosis, or treatment. blood-test.life is not a medical device. Always consult your physician or a qualified health provider about your results. Read our full medical disclaimer.