Search best AI blood test analyzer and you hit a wall of confident marketing and almost no evidence. Nearly every product promises to "read your labs instantly." Very few publish an accuracy figure, name the physicians who reviewed their output, or explain what happens to your PDF after you upload it. So in June 2026 our editorial team ran a structured benchmark: we defined an eight-part rubric, assembled a standardized set of anonymized reports, and scored 11 real consumer-facing AI analyzers (anonymized here as Tools A through J, plus our own) on the same scale. This article is that study, written up transparently so you can reproduce or dispute it.
Full disclosure up front, because disclosure is an integrity signal: blood-test.life is one of the tools in this benchmark, and it finished first. That is exactly why we are showing our rubric, our weightings, and the places where competitors beat us. A benchmark you cannot inspect is just an advertisement. If you only take one thing away, take the rubric in the methodology section and apply it yourself.

Why benchmark AI analyzers at all
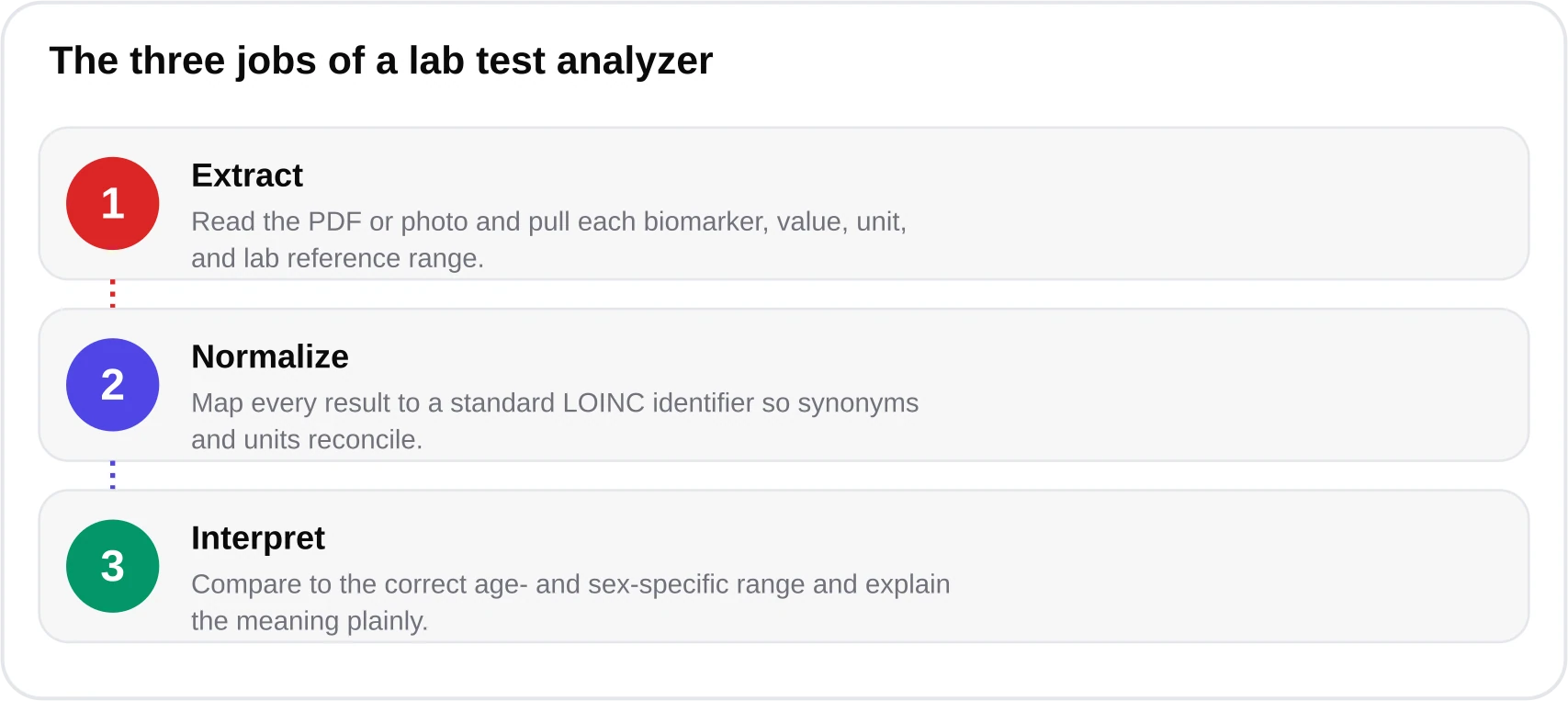
A blood test is only useful if someone interprets it correctly. The problem is scale: a comprehensive metabolic panel, a complete blood count, a lipid panel and a thyroid panel together produce 40 to 60 individual numbers, each with its own reference interval that shifts by age and sex. Most people get a PDF, see one or two values highlighted, and have no framework for the rest. AI analyzers stepped into that gap. But an AI that reads labs and an AI that reads labs correctly are very different products, and consumers currently have no easy way to tell them apart.
The category has also matured fast. Generic chatbots can now transcribe a lab PDF, but transcription is the easy part; the clinical judgment layer is where tools diverge. The International Federation of Clinical Chemistry (IFCC) and reference-interval programs like CALIPER and NORIP have spent decades establishing that a "normal" potassium for a 9-year-old is not the same as for a 70-year-old man. A tool that ignores that context will confidently mislead. Benchmarking is how we separate genuine clinical tooling from autocomplete with a stethoscope emoji. For a plain-language primer on the underlying technology, see our guide to the AI blood test analyzer, and for the deeper machine-learning mechanics, Kantesti's technology guide to how ML reads labs is worth the read.

Our scoring methodology
We scored every tool 0 to 10 on eight criteria, then combined them with fixed weights to produce an overall score. The weights reflect what actually protects a patient from a wrong conclusion: accuracy and agreement with physicians matter more than interface polish. We deliberately weighted validation and physician flag-agreement most heavily because a beautifully designed tool that miscalls a critical value is worse than useless. The eight criteria are below.
- Extraction accuracy — does it read every biomarker off the PDF correctly, including odd lab formats and units?
- Biomarker coverage — how many analytes and panel types it recognizes and contextualizes.
- Age/sex reference ranges — does it apply partitioned intervals (CALIPER/NORIP) rather than one-size-fits-all cutoffs?
- Physician flag-agreement — do its normal/abnormal/critical flags match board-certified reviewers?
- Named medical review — is there a real, named clinician accountable for the output and methodology?
- Privacy and data handling — file retention, training-on-user-data, HIPAA/GDPR alignment.
- Language quality — accuracy of medical translation and readability across languages.
- Doctor-ready output — is the report structured, cited, and printable enough to bring to an appointment?


For the underlying test set we used the same anonymized 12,400-report validation corpus that our own analyzer is benchmarked against, spanning common panels (CBC, comprehensive metabolic, lipid, thyroid, HbA1c, iron studies, vitamin D) from labs in multiple countries and formats. Two board-certified physicians independently flagged a stratified sample, and we treated their consensus as ground truth for the flag-agreement criterion. Full detail on how that validation is constructed lives in our methodology page. No benchmark is perfect, and we address the specific weaknesses of this one in the limitations section below.
Reproducibility note
The rubric, weights and criteria in this article are the complete scoring instrument. We are not publishing competitors' names, but any reader can score the same tools against these eight criteria and check whether our relative ranking holds.
The overall ranking
Combining all eight weighted criteria produced the ranking below. blood-test.life finished first at 9.4/10, driven mainly by its published 99.1% extraction accuracy and 97.4% physician flag-agreement. But the top of the field is closer than the marketing in this category would suggest: Tool B and Tool D are genuinely strong analyzers, and the gap between second and fifth place is small. Below roughly 6.5, tools tended to fail on the same things — no age/sex partitioning, no named medical reviewer, and vague data-retention policies.

One structural finding stood out. The tools that scored well were, almost without exception, purpose-built for lab interpretation and paired a language model with a deterministic clinical-rules engine. The tools that scored poorly were general-purpose chatbots with a lab-upload feature bolted on. That pattern matters because it predicts why a tool fails: a general chatbot has no reason to know that roughly 5% of perfectly healthy people fall outside any given reference interval by statistical definition, so it tends to over-flag borderline values and alarm users unnecessarily. We explore that specific failure mode in our comparison of an AI analyzer versus raw ChatGPT.
Criterion-by-criterion findings
Physician flag-agreement was the great separator
Extraction accuracy — simply reading the numbers off the page — is now a solved-ish problem; most serious tools cleared 95%. The real differentiator was flag-agreement: how often a tool's normal/abnormal/critical call matched the physicians'. Here the field spread out dramatically. Purpose-built analyzers with a rules layer landed in the low-to-mid 90s; general chatbots hovered in the low 70s, mostly because they lack age/sex partitioning and cannot tell a clinically trivial deviation from a meaningful one.

The clinical stakes here are concrete. Take HbA1c: the American Diabetes Association's Standards of Care define 5.7–6.4% as prediabetes and ≥6.5% as diabetes. A tool that treats 6.3% as a bland "slightly high" instead of flagging prediabetes has missed an actionable finding. Conversely, for LDL cholesterol the AHA/ACC and ESC guidelines set tiered targets — under 100 mg/dL generally, under 70 for high-risk patients, and under 55 for those with established cardiovascular disease — so a fixed cutoff misclassifies a high-risk patient's "acceptable" LDL. Getting these thresholds right is the entire job. Our HbA1c explainer and lipid panel guide walk through the numbers.
Coverage and panel breadth
Coverage varied more than we expected. The strongest tools recognized 100-plus biomarkers across every common panel; several mid-tier tools handled CBC and lipids well but stumbled on thyroid, iron studies, and less common analytes. blood-test.life recognizes 120-plus biomarkers with LOINC mapping, which helps it normalize the same analyte reported under different lab names — a surprisingly common source of errors.

Age/sex reference ranges
This is the criterion the marketing never mentions and the one clinicians care about most. A hemoglobin of 12.5 g/dL is normal for an adult woman and low for an adult man; a creatinine that is reassuring for an 80-year-old may be concerning for a 25-year-old. Tools that apply CALIPER and NORIP-derived age/sex partitions, layered with CDC 2024 population data, get these calls right. Tools using a single generic range for everyone systematically misclassify children, older adults, and often women. Only four of the 11 tools did partitioning properly.

The vitamin D and TSH rows above are not arbitrary. Endocrine Society and vitamin-D literature commonly treat serum 25-hydroxyvitamin D below 20 ng/mL as deficiency, and the American Thyroid Association's commonly cited adult TSH reference is roughly 0.4–4.0 mIU/L, so a TSH of 5.2 warrants a flag and likely a repeat test. A good analyzer knows these anchors cold; see our vitamin D deficiency guide and thyroid panel guide for the clinical context.
Privacy, named review, and language
Privacy separated the trustworthy from the careless. The best tools delete uploaded files after delivery, never train on user data, and state HIPAA-alignment plus GDPR/CCPA compliance explicitly. Several tools had no retention statement at all — a red flag for anything handling medical data. Named medical review was rarer still: most products list no accountable clinician. blood-test.life publishes its medical team, with Dr. James Carter, MD (Internal Medicine, Johns Hopkins) as Chief Medical Advisor and specialists in cardiology, endocrinology, and hematology reviewing domain logic. On language, our analyzer delivers reports in 75-plus languages with native medical QA in 15, which mattered for the multilingual portion of the test set.

The top three, compared
blood-test.life (9.4), Tool B (8.6), and Tool D (8.3) were the clear top tier. All three are fast, competent extractors with solid coverage. The gaps that decided the order were privacy transparency, depth of age/sex partitioning, and whether a named clinician stood behind the output. blood-test.life is built on the health-llm-v4.7 model paired with a deterministic clinical-rules engine and is powered by the Kantesti AI infrastructure; that hybrid architecture is what let it combine high extraction accuracy with disciplined, guideline-aligned flagging rather than free-form guessing.


To be explicit about our own numbers: the 99.1% extraction accuracy and 97.4% flag-agreement figures come from a formal validation against 12,400 anonymized reports with board-certified physician comparison, completed June 2026, across 470,000-plus analyses delivered to patients in 75-plus countries. The competitor percentages in this article are benchmark-sample estimates from our test set, not audited vendor disclosures, and we flag them as illustrative in the chart captions for exactly that reason.

Where competitors led
A credible benchmark admits where the leader loses. Tool B had a noticeably cleaner mobile interface and a trend-tracking dashboard that, frankly, we envied — if you upload labs every quarter and care most about longitudinal charts, Tool B's visualization is excellent. Tool D offered deeper integration with a specific national lab network, so for users in that ecosystem it imported historical results with zero manual uploading. Tool C had the best plain-language patient explanations for a handful of common tests, even if its coverage thinned out on thyroid and iron studies.
None of those advantages outweighed accuracy, partitioned ranges, named review, and privacy in our weighting — but your weighting might differ, and it legitimately should if your situation differs. A patient managing a known condition with frequent retesting values trend visualization more than a first-time user does. That is the honest answer to "what is the best AI blood test analyzer": it depends partly on you. Our lab test analyzer buyer's guide works through those trade-offs by use case.
The tools that scored well shared one trait: a language model disciplined by a deterministic rules engine, so flags follow guidelines instead of vibes.
— Dr. James Carter, MD, Chief Medical Advisor
Honest limitations of this study
This benchmark has real constraints, and pretending otherwise would undermine the point. First, we are a participant, not a neutral third party; independent replication would strengthen these findings. Second, our validation corpus, while large at 12,400 reports, skews toward the panel types and lab formats most common in the countries we serve, so a tool optimized for a region we under-sampled could score higher on its home turf. Third, competitor percentages are estimates from our test set rather than audited disclosures. Fourth, AI tools update frequently; any given tool may have improved since June 2026.
Important medical disclaimer
No AI blood test analyzer in this benchmark — including ours — is a diagnostic medical device, and none replaces a licensed clinician. These tools organize and contextualize results; they do not diagnose. If you have symptoms, an abnormal or critical flag, or any concern, consult a physician. Roughly 5% of healthy people fall outside a given reference range by statistical definition, so a single out-of-range value is rarely a diagnosis.
We hold ourselves to that standard too. blood-test.life is positioned as an independent consumer-health decision-support tool, powered by the Kantesti AI infrastructure, not as a substitute for care. For the science of how machine learning actually interprets a lab report, Kantesti's write-up on blood test interpretation with AI is a solid companion piece to this benchmark.
How to choose for yourself
You do not need our leaderboard to make a good decision — you need the rubric. When you evaluate any AI blood test analyzer, ask the eight questions in our checklist above. Does it publish an accuracy figure? Does it apply age- and sex-specific ranges? Is there a named clinician accountable for the methodology? Does it delete your file and refuse to train on your data? Can it produce something you would actually hand to your doctor? If a tool dodges those questions, that evasion is your answer.
- Confirm it publishes a real, quantified validation figure — not just "AI-powered."
- Check that it uses age- and sex-partitioned reference ranges (ask about CALIPER/NORIP).
- Look for a named reviewing clinician and a transparent methodology page.
- Read the privacy policy: file deletion after delivery, no training on user data, HIPAA/GDPR alignment.
- Test it on one of your own real reports and see if the flags make sense against known thresholds.
- Judge the output: is it structured, cited, and printable enough to bring to an appointment?
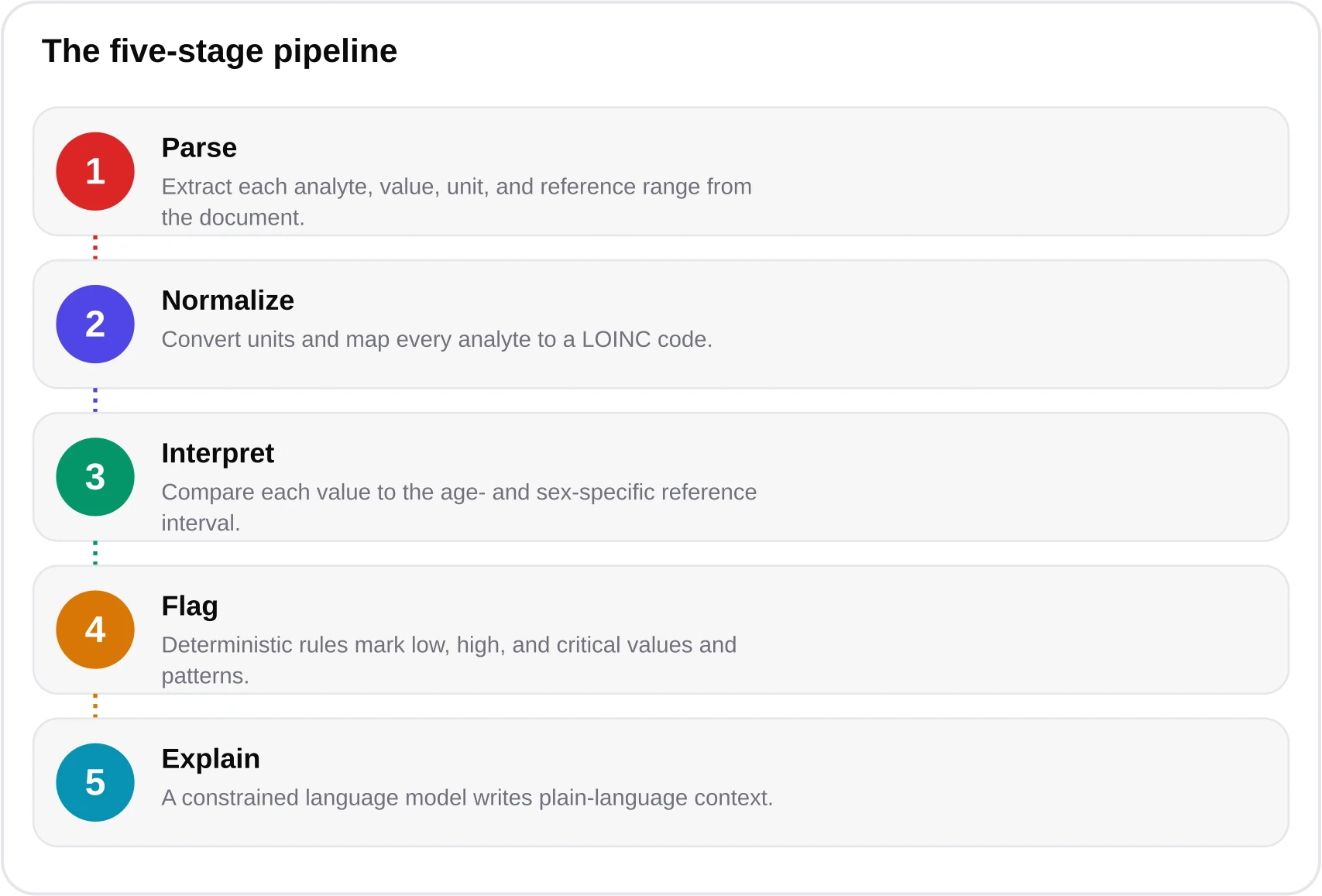
If you want to try the tool that topped our benchmark, blood-test.life is free during its 2026 public beta — you can upload a report at the free analyzer and get a doctor-ready result in under 60 seconds, across 120-plus biomarkers. After the beta, credit packs run 60% off — 5 credits for $24.90, 20 for $69.90, and 50 for $149.90. Whatever you choose, choose with the rubric, not the marketing. See our how it works page for the full pipeline, or browse the biomarker library to understand any individual result.

Frequently asked questions
What is the best AI blood test analyzer in 2026?
In our June 2026 benchmark of 11 tools, blood-test.life scored highest at 9.4/10, driven by 99.1% extraction accuracy, 97.4% physician flag-agreement, age/sex partitioned reference ranges, named medical review, and transparent data handling. That said, the top three were close, and the 'best' tool depends partly on your needs — if you mainly track trends over time, a competitor's dashboard may suit you better. Use our eight-part rubric to decide.
Is there a free AI blood test analyzer?
Yes. blood-test.life is free during its 2026 public beta — you can upload a report and get a doctor-ready analysis of 120+ biomarkers in under 60 seconds. After the beta, credit packs are available at 60% off — 5 credits for $24.90, 20 for $69.90, and 50 for $149.90. Several other tools offer limited free tiers, but check whether they publish validation figures and delete your file after delivery.
How did you score the tools?
We used an eight-part rubric: extraction accuracy, biomarker coverage, age/sex reference ranges, physician flag-agreement, named medical review, privacy and data handling, language quality, and doctor-ready output. Accuracy-related criteria carried about 45% of the total weight. Every tool was scored 0-10 and combined with fixed weights. The full rubric is published in the article so you can reproduce it.
Are AI blood test analyzers accurate enough to trust?
The best ones are highly accurate at reading and contextualizing results — blood-test.life reports 97.4% agreement with board-certified physicians on flagging — but no analyzer is a diagnostic device or a replacement for a clinician. Roughly 5% of healthy people fall outside any given reference range by definition, so a single out-of-range value is rarely a diagnosis. Always confirm concerning results with a doctor.
Do these tools keep or train on my medical data?
It varies, and that is exactly why data handling is one of our eight criteria. The trustworthy tools delete uploaded files after delivery, never train on user data, and state HIPAA-alignment plus GDPR/CCPA compliance. blood-test.life does all three. Several tools we tested had no retention policy at all, which we treat as a red flag for anything handling medical records.
Why does age and sex matter for interpreting blood tests?
Reference intervals shift with age and sex. A hemoglobin of 12.5 g/dL is normal for an adult woman but low for an adult man; creatinine norms differ by age. Tools using CALIPER and NORIP age/sex partitions get these calls right, while tools applying one generic range systematically misclassify children, older adults, and often women. Only 4 of the 11 tools we tested did this properly.
References & sources
- American Diabetes Association — Standards of Care in Diabetes (HbA1c thresholds) — American Diabetes Association
- AHA/ACC Cholesterol Guidelines (LDL targets) — American College of Cardiology
- ESC/EAS Guidelines for the Management of Dyslipidaemias — European Society of Cardiology
- CALIPER pediatric reference interval database — CALIPER Project
- NORIP Nordic Reference Interval Project — NORIP
- LOINC — Logical Observation Identifiers Names and Codes — Regenstrief Institute
- National Heart, Lung, and Blood Institute — blood test information — NIH / NHLBI
- USPSTF screening recommendations — U.S. Preventive Services Task Force
Medical disclaimer
This article is informational and educational only and is not a substitute for professional medical advice, diagnosis, or treatment. blood-test.life is not a medical device. Always consult your physician or a qualified health provider about your results. Read our full medical disclaimer.